For the first time since it was first detected almost three years ago and ravaged Nepal, the SARS-CoV-2 virus has been overtaken by another public health emergency: the dengue epidemic.
Covid-19 is not gone (even President Bidya Devi Bhandari just had it), and new strains are co-mingling with various serotypes of dengue that have officially claimed 39 lives and infected over 30,000 people across Nepal this monsoon. But like the numbers for Covid-19, those are gross under-estimations.
As we speak, a new Omicron sub-variant BF.7 which is better equipped to escape antibodies from earlier infections or vaccinations has already spread from the United States to China. Masks, bivalent boosters and avoiding crowds are the most effective prevention methods which only a few follow.
Yale University researchers have found considerable growth in excess deaths (total deaths in a population in a given period which is above what is normally expected) among anti-vaxers in Ohio and Florida.
In fact, the fatality rate seems to have a direct correlation with political belief. The paper published by the National Bureau of Economic Research this month showed that excess death rates for American republicans increased from nearly 0% pre-pandemic to 35% by end-2021. The increase for Democrats was only 10%.
Similarly, another study published in The Journal of the American Medical Association last month revealed that Covid hospitalisations in 13 US states was 10.5 times higher among the unvaccinated and 2.5 times higher in vaccinated persons with no booster shots.
Closer home, Hong Kong saw a disproportionate number of Omicron deaths earlier this year among the unvaccinated elderly. While highly transmissible, the strain was much less fatal among the vaccinated elsewhere.
Even in Nepal, which has a full vaccination rate close to 80%, one of the highest in the world, those still being hospitalised with Covid were mostly unvaccinated.
“I recently had a girl patient who had lost her parents and a brother to Covid who had not been vaccinated,” recalls Sher Bahadur Pun, a virologist at Teku Hospital in Kathmandu. “There have been one too many unvaccinated patients in my ICU who believed rumours on social media.”
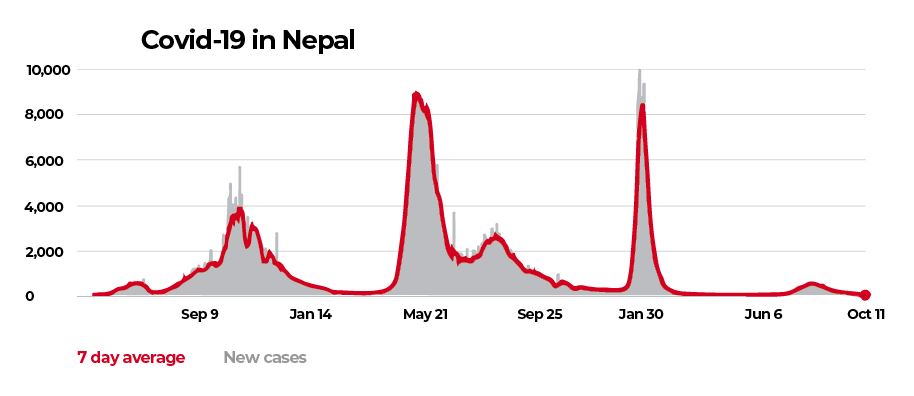
In Nepal, as elsewhere, the early days of the pandemic were marked by rampant misinformation, first about the novel coronavirus itself, stigmatisation of patients and healthcare providers alike. The general public was slow to adopt safety protocols, which contributed to over 1 million cases and 12,000 deaths in Nepal. Worldwide, there have been over 630 million cases and at least 6.5 million deaths from Covid so far.
The pandemic did reinforce hand washing, hygiene and mask-wearing in Nepal, which in turn also helped reduce incidences of tuberculosis, typhoid, flu and other infectious diseases.
But the biggest disruption was caused by repeated lockdowns which led to an economic crisis in Nepal, lately worsened by the Russian invasion of Ukraine. All this has slowed improvements in nutrition levels as well as maternal and infant health.
During the pandemic, Nepal had an early warning of what was to come just by following trends in neighbouring India (see book review, below). But lack of adequate preparation at the border meant ineffective quarantine and testing, and a rapid spread of the virus to the remotest corners of the country. As hospitals in India ran out of beds and oxygen, so did Nepal.
The second wave in 2021 saw India register the highest daily Covid-19 deaths, but the death rate proportional to population was probably higher in Nepal. Better-equipped hospitals with trained staff and adequate oxygen and ICU facilities across the country would have saved many of those lives.
“Countries like Nepal will have to prepare for not just new emerging diseases but also re-emerging and existing infections. And the only way to do that is by strengthening our health system,” adds Pun “We must start training our medical personnel and upgrade health infrastructure. That is the biggest takeaway from the pandemic.”
Nepal was one of the first countries to volunteer for Oxford University’s Recovery Trial which studied the efficacy of various drugs, yet there is rampant over-prescription and over-the-counter availability of antibiotics.
“We are still using antibiotics like Azithromycin to treat viral infections such as Covid and dengue which is adding to the problem of antimicrobial resistance,” says Buddha Basnyat, a physician at the Patan Academy of Health Sciences.
At Teku Hospital, many of virologist Sher Bahadur Pun’s patients are also testing negative for dengue and suspects the mosquitoes that bit them could have been carrying another virus like Zika or Chikungunya which have been detected in India. "The symptoms are very similar and transmitted by the same mosquito," he adds.
Covid-19 is just one of many pandemics. But it won’t be the last. As humans interact with a deteriorating natural habitat and wildlife, they are exposed to zoonotic diseases — viruses that can jump from animals to humans. The growth in instantaneous international travel means infections can spread rapidly across the world.
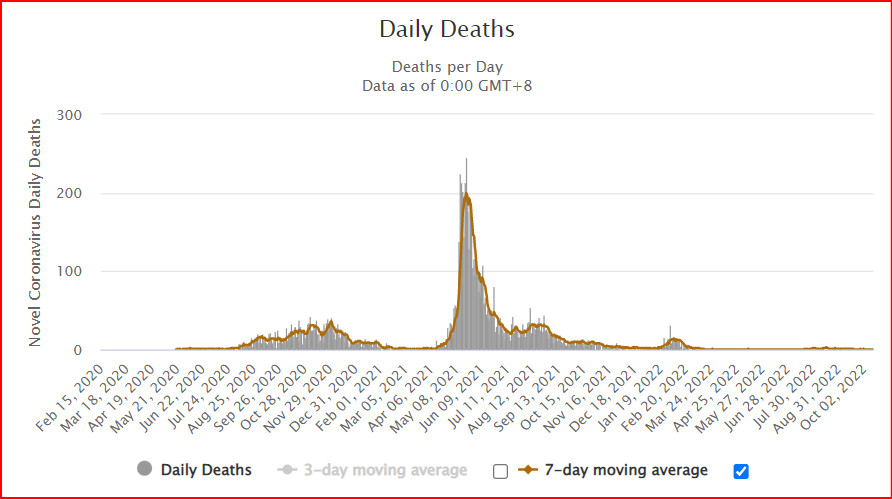
At the peak of the second wave with the Delta strain more than 250 Nepalis were dying every day, but governments in Kathmandu and the provinces were preoccupied with a nasty power struggle. Political infighting delayed response, and led to many more unnecessary deaths.
As Nepal and India prepare to mark the third year of the Covid-19 outbreak, the worst seems to be over. It took a global crisis and millions of deaths to remind us to be prepared for the next pandemic.
Says Buddha Basnyat: “We now have to make the best use of our capacity and build on it. Let’s not be complacent, there are many other infections that afflict this part of the world.”

Pandemic unmasked the real disease: governance failure
On 24 March 2020, the Narendra Modi government in India imposed the first lockdown with just four hours of warning. WHO praised this ‘timely and tough action’ to stop Covid, and the University of Oxford at the time called it the strictest lockdown in the world. With China’s zero-Covid policy that is probably not true anymore.
Still, India’s sudden lockdown unleashed the greatest movement of people in the Subcontinent after the 1947 Partition, which had a cascading effect on Nepal.
‘For a country with zero social security, which did not even have an authentic count of the number of people left without an income due to the lockdown, and where fractiousness and social fault lines make the poor and the backward easy preys of the systematic corruption, a measure like this would need weeks of planning. Even then it could still go wrong. So the repercussions of such a move without any preparation were unimaginable.’
In her book Billions Under LockdownIndian journalist Abantika Ghosh chronicles the impact of lockdowns on her country. In a smaller scale, the upheavals caused by the lockdowns impacted Nepali migrant workers in India and Indians in Nepal who had to undertake arduous treks home.
In her book, Ghosh tells the story of 38-year-old Ranveer trying to make the 400km journey on foot from Delhi to his village in Madhya Pradesh. He died along the way, 100m short of reaching his destination. Nepali migrant workers, prevented from entering their own country at the border, swam across the Mahakali River in Darchula. Some drowned.
Once quarantined, often without proper testing and contact tracing, Covid refugees were housed in crowded shelters which themselves became super-spreaders for the virus. The outbreak snowballed as migrants took the virus home to families, leading to community transmission.
As hospitals were overwhelmed with cases, several treatment therapies were introduced. From a combination of HIV drugs and convalescent plasma therapy to malaria drug hydroxychloroquine, a typhoid antibiotic Azithromycin and Remdesivir, all of which were later proven to be ineffective, and sometimes even harmful. What saved lives was the timely supply of oxygen, and the cheap steroid Dexamethasone.
Ghosh writes about India: ‘The biggest lesson of all was how politics became the most insurmountable impediment in the control of the disease.’ Ditto for Nepal.
The pandemic unmasked the real disease: state neglect, corruption, governance failure leading to ad-hoc restrictions, lack of testing and surveillance, an overwhelmed health system that left hundreds of millions of hapless citizens to fend for themselves.
It also showed what worked: empowered local health institutions which responded quickly with testing, tracing and quarantining. No surprise that the Indian state with the lowest Covid fatality rate despite high exposure was Kerala.
Abantika Ghosh’s lessons learnt could just as well be written for Nepal: ‘A matured health system is also decentralized, transparent, and, on occasion, self-sustaining … If you don’t treat diseases early, you only treat them when they are complex, and because complex interventions are more expensive, you do not have the resources left to bolster primary care. The more hospitals you build without investments in primary care, the more hospitals you will need to build.’
Sonia Awale
Billions Under Lockdown: The Inside Story of India's Fight Against Covid-19
By Abantika Ghosh
2021 Bloomsbury
IRS699
393 pages