

This op-ed is being simultaneously published in the Indian Express (India), The Daily Star (Bangladesh), Nepali Times (Nepal) and DAWN (Pakistan).
In February 2021, Covid-19 numbers started increasing again in South Asia with official daily case counts rising beyond 400,000 in India, 6,000 in Pakistan and 7,500 in Bangladesh, straining health systems.
The massive surge in India soon spilled over across the border into Nepal, leading to ‘apocalyptic’ scenes of overwhelmed hospitals.
This virus knows no borders. Containing it has necessitated global cooperation among scientists, policy makers and society. Despite a wide variation in how nations have responded to the pandemic, the most successful strategies adhere to science, and attention to local context.
The deadly surge in 2021 makes a regionally-coordinated, evidence-driven strategy even more critical. The virus continues to challenge us with its mutations and new lines of attack. If we are to move at the speed of the virus, it is necessary to construct multi-stakeholder regional coalitions to devise new solutions and frugal innovations that can be applied across South Asia.
Given our shared and mostly similar social, economic and cultural contexts, local successes must find means to be amplified across the region.
Is that even possible, given the troubled history South Asian countries share? The mutual mistrust appears to have hit a new low, as SAARC has not even managed to hold its summit since 2014.
But today we write a positive, hopeful story about a new consortium we are involved in, with core team members from India, Pakistan, Nepal, and Bangladesh jointly developing Covid prevention strategies. The emerging consortium provides an example of how neighbours can work together for mutual benefit, despite political differences.
Every country in South Asia has struggled to ensure consistent mask-wearing to stem the spread of Covid. Beliefs, priorities, traditions, and aversions to behaviour change are more similar across South Asia than we care to admit. These commonalities mean that interventions that are successful in changing behaviour in one place are likely applicable in other parts of the Subcontinent.
We have experienced this with Community-Led Total Sanitation (CLTS) campaigns to solve the problem of open defecation -- originally developed by Bangladeshi NGOs in partnership with an Indian consultant --- and now broadly applied across South Asia and beyond.
The Grameen Bank microcredit model was an indigenous South Asian innovation that spread rapidly. BRAC’s recent ‘Graduation’ program targeting the ultra-poor in Bangladesh was replicated with success in India and Pakistan. India’s digitised social protection ecosystem with Aadhar IDs and Jan Dhan accounts serves as a model (albeit with cautionary notes) for other countries in the region. E-governance programs in Pakistan, like eVaccs and Citizen Feedback Model have been replicated and provide strong models ready to be deployed regionally and globally.
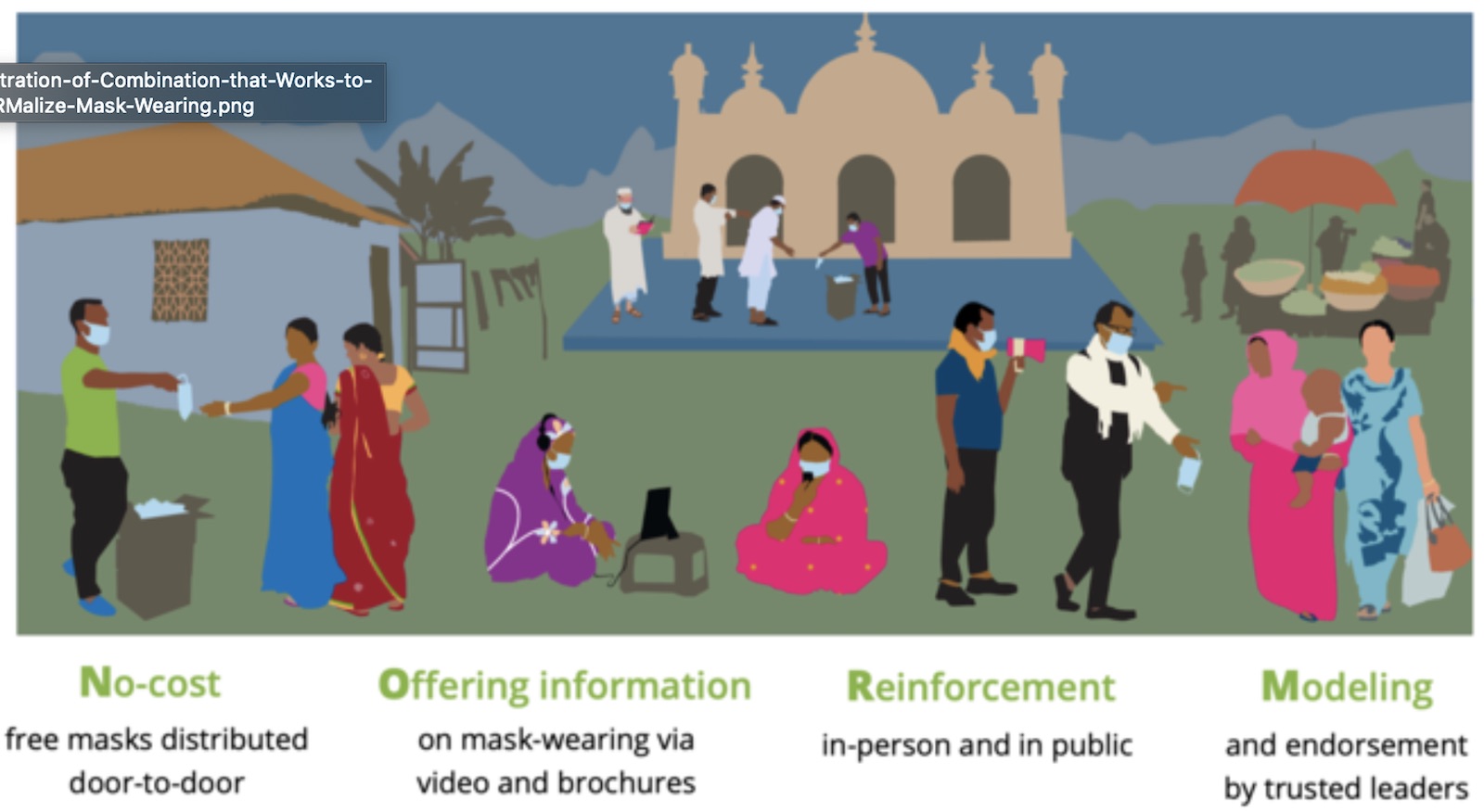
The new pan-South Asian consortium in response to Covid-19 evolved out of an experiment conducted in Bangladesh, that successfully changes social norms around mask-wearing in rural communities. We observed that a combination of No-cost distribution, Offering information, Reinforcing the message in markets, mosques and other public spaces, and Modelling and endorsement by community leaders (NORM) leads to large, sustained increases in mask usage that persisted beyond the period of active intervention.
This four-part NORM intervention was originally examined in a cohort of 350,000 individuals across 600 villages. BRAC is implementing the model to reach 81 million people across Bangladesh.
The team is now partnering with several organisations across Pakistan, India, Nepal, and Bangladesh to start adapting the model to fit each country’s context, and set up partnerships to pilot, implement, tinker, and learn.
The Self Employed Women’s Association (SEWA) quickly implemented the model to reach over one million members in Gujarat. An additional 1.5 million masks were shipped from Bangladesh to support SEWA’s outreach to other states. Lahore’s Commissioner worked with our research team to adapt the NORM model to an urban setting, and devised new creative ideas to improve effectiveness.
For example, it has prepared to deliver masks at doorsteps using Pakistan’s postal service, and is targeting beneficiaries on the basis of billing information from utility companies. Philanthropists and private corporations are sponsoring the masks. We are re-importing some of these innovations back to Dhaka, inspiring further scale-ups in Dhaka, Chittagong, Rajshahi and Kathmandu.
Effective mask promotion requires visits to thousands of remote villages, and those same visits can be used to prepare for more effective community-based healthcare responses. To that end, a host of physicians, scientists and community based organisations created the Swasth Community Science Alliance, committing to pragmatic, science-based protocols to manage mild and moderate cases of Covid-19 in rural India, where institutional health care access is limited.
These guidelines (available at https://science.swasth.app) were translated to training tools for healthcare workers by digital health innovators like Noora Health, making them widely available across the region.
NORM implementation teams based in Lahore, Ahmedabad, Peshawar, Hyderabad, Dhaka, Kathmandu, and Delhi are learning from each other’s successes and failures. The process usually starts with the original research team sharing evidence-based insights with implementing agencies, as the implementers adapt the design, co-create localised implementation protocols, and are threaded together in a collaborative environment across countries where each implementing team iterates while learning from others’ prior iterations, and all our sub-teams are connected in an active learning system that allows us to course-correct in real time. This coalition is poised to change mask-wearing norms amongst hundreds of millions of people across all of South Asia.
The CSA is working with partners across rural, tribal belts around India. A team of physicians from India and the Indian diaspora work with local implementing partners to support design, implementation and monitoring of home-based programs and Covid-19 centres providing rigorously protocolised treatment for moderate cases, with oxygen, proning and steroids.
Combining the NORM and CSA interventions, our Masking-Treatment-Vaccine Preparation (MTV) approach offers a sensible strategy to mitigate the pandemic until universal vaccination is achieved. These are regional solutions that thoughtfully apply scientifically sound interventions to the local context.
The Covid-19 crisis has increased policymakers’ appetite for evidence-informed policy measures that can be quickly implemented to stem transmission. This drive for quick action has created some unprecedented opportunities for enhanced cross-country collaborations that are normally hampered by politics and mistrust.
We hope that the consortium that first formed around mask-promotion, and now around science-based treatment approaches, and that developed quickly and organically without regard to national boundaries, can serve as a model for a broader and deeper collaborative ecosystem that endures.
We need to come together to solve problems that affect us all. Let the lasting legacy of this pandemic be a new era of partnership in social innovations that can benefit all South Asians.
Mushfiq Mobarak is Professor of Economics, Yale University, and Director of the Yale Research Initiative on Innovation and Scale. Twitter: @mushfiq_econ
Maha Rehman is director of policy at the Mahbub-ul-Haq Research Centre at the Lahore University of Management Sciences. Twitter @MahaRehman1
Satchit Balsari is assistant professor of emergency medicine, and of global health and population, at Harvard University. Twitter: @satchit_balsari