
Like every monsoon, this year has also seen a spike in snakebite deaths across the country. In the Tarai, emergency wards are crowded with patients as doctors try to cope. At least 15 people have died so far in Saptari, Sarlahi, Morang and Rautahat, districts that were also hardest hit by floods last month.
There are at least 40,000 cases of snakebite every year in Nepal, with some 3,000 fatalities in the Tarai alone. But a recent epidemiological study found the death rate from snakebite has come down from 18.7% 20 years ago to 6.62%, largely because of awareness and anti-venom treatment.
Read also: "Snakebite is treatable, no one need die from it."
Globally, 5.5 million snakebites occur every year, with up to 138,000 deaths. Another 400,000 people require amputations and suffer severe injuries. Bangladesh, India, Nepal, Pakistan and Sri Lanka together account for 70% of global snakebite mortality. But it was not until 2017 that the World Health Organisation (WHO) recognised snakebite as a neglected tropical disease, and came up with a roadmap to reduce risk.
In Nepal too, snakebite never received the attention it deserved. It is not communicable or infectious, is rare and tropical and affects the poorest people.
“Snakebite is a severely neglected public health burden in Nepal. There is so much we don’t know about snakes and their venoms, and there are signs it is going to get worse with climate change,” warned Sher Bahadur Pun of Sukraraj Tropical and Infectious Diseases Hospital in Kathmandu. (See box)

High Level Meeting and Workshop on Snakebite in Nepal on 2-3 August in Kathmandu, is the first international conference on snakebite in the country. Taking part are 20 of the world's foremost authorities on snakebite including David Warrell of Oxford, David Williams, head of the Global Snakebite Initiative (see interview, page 7), Ulrich Kuch of Goethe University in Frankfurt, and Priyanka Kadam from India, and 50 Nepali scientists are taking part.
Nepal is aiming to be one of 11 member countries on WHO’s roadmap for snakebites, and is trying to muster serious commitment from the government for research and treatment.
“We hope to sensitise policymakers and the public about the hidden burden of this neglected tropical disease,” said Sanjib K Sharma, a doctor at the BP Koirala Institute for Health Science in Dharan, one of the conference organisers. “We also want to start working on developing anti-venoms in Nepal instead of depending on imports.”
Of the four types of anti-venom imported for the 21 types of poisonous snakes in Nepal, one doesn’t work and three others are not reliable. In fact, 80% of people here who are administered anti-venom suffer from reactions, 12% of which are fatal. Activists in India are now lobbying to stop the export of anti-venom because of unmet domestic need.
Anti-venom is produced by injecting donor animals such as horses and sheep with venom, and then extracting the antigen from the blood. But the procedure is expensive – a vial of anti-venom costs up to $2,200. Since snakebite requires between 20-25 vials to neutralise the venom, the pharmacy bill alone would total $30,000 per patient. Global production is limited, and most snake bites can only be cured with anti-venom from that particular species.
WHO’s target is to halve the numbers of deaths and disability from snakebite by 2030, and the Wellcome Trust and UK Department for International Development (Dfid) have announced £80 million and £9 million respectively for the development of a universal anti-venom. However, clinical trials will take decades.
Nepal’s challenge is at ground level. Awareness about preventing snakebite is still low, people prefer to visit traditional healers if bitten, and many patients get to anti-venom centres too late. Even so, snakebite fatalities fell from 10.5% to 0.5% after motorcycle volunteers were deployed in a pilot project in 2013. (see box)
Diana Barr of the Australian Venom Research Institute at the University of Melbourne says Nepal and Bangladesh are best equipped to take the WHO strategy forward. “You’ve got some of the key things, like local expertise, your health ministry is pushing for change, and there is support from outside organisations,” she told Nepali Times. “Nepal can easily implement the WHO strategy and get dramatic results in a couple of years.”
Experts attending the Kathmandu conference this weekend believe the WHO target of halving snakebite deaths is doable. All it needs is effective treatment, trained nurses and doctors who deliver that treatment, educating the community to take simple precautions, and come to hospitals sooner if bitten.
Said Sharma of BPKIHS: “The universal vaccine is the holy grail for snakebite treatment, but until then we have to work on anti-venom epidemiology within the country and educate people about snakebites.”
Motorcycle volunteers to the rescue

One of the major barriers to snakebite treatment is the delay in getting victims to a health centre with anti-venom. In many cases, patients die on the way due to an inefficient transportation system.
In 2004, a group from BPKHS in Dharan, in collaboration with the University of Geneva, tested a Motorcycle Volunteer Program in four villages in the eastern Tarai with a high incidence of snakebites.
The pilot project mobilised motorcycle volunteers in all four villages, which had a total population 62,000. They helped transport snakebite victims to a specialised treatment centre in Damak that had anti-venom and staff trained in snakebite management. The motorcycles combined with community health education sharply reduced the mortality rate from snakebite.
Before the experiment, there were 502 bites/100,000 population with a case fatality rate of 10.5%. After the intervention, the incidence decreased to 315 bites/100,000 and the fatality rate fell to 0.5%.
‘Simple educational messages and promotion of immediate and rapid transport of victims to a treatment centre decreased the mortality rate and incidence of snake bite in southeastern Nepal,’ stated a study published in The American Society of Tropical Medicine and Hygiene in 2013. It recommended that the test be replicated elsewhere.
Snakes and Ladders
As global temperatures go up, so do snakes, insects and plants. Not only are venomous snakes now found at altitudes where they were not present before, experts say even their venom may be getting more poisonous.
Kathmandu Valley used to experience snake bites, but they were never fatal. Now, there are cobra sightings on the Valley rim, and even in Langtang National Park. And last year, a patient admitted for snakebite at Sukraraj Hospital in Teku died while undergoing treatment.
Poisonous snakes may have come up hitchhiking on cargo trucks carrying logs from the Tarai, but health experts say there is evidence climate change may be allowing venomous snakes, and other tropical wildlife, to move to higher areas of the Himalaya.
“Elsewhere we are starting to see the movement of various species with the warming of the earth, so the case of snakes should be no different,” explains Sher Bahadur Pun of Sukraraj Topical and Infectious Disease Hospital in Kathmandu, which has seen a rise in the number of patients from the Valley and surrounding districts with severe snakebites.
Pun adds that more research needs to be done to find the exact correlation between venomous snakes and climate change.
In addition, snakebites that were previously poisonous only in the immediate tissue surrounding a bite can now be more venomous or even fatal. A warmer climate appears to affect the physiology of the venom glands and the chemical composition of snakes' secretions.
“When people got bitten by snakes in the past, they only developed swelling, but now I see cases where victims are bleeding from bites by the same type of snake,” says Sanjib K Sharma of the Department of Internal Medicine at BPKHS in Dharan.
Read also: Snakebite!, Buddha Basnyat
An ounce of venom, Buddha Basnyat
Snakebite is treatable, Nepali Times
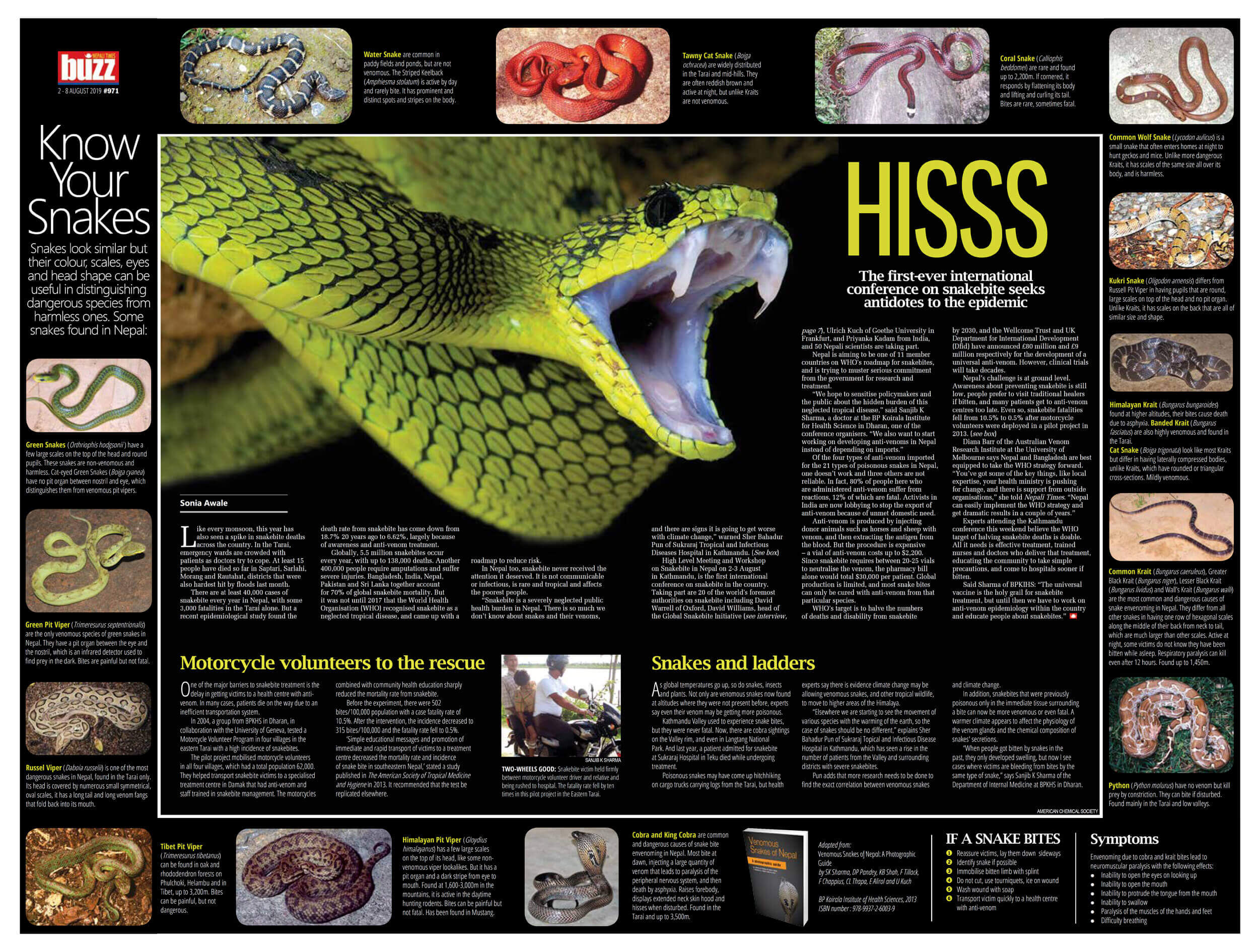
Know Your Snakes
Snakes look similar but their colour, scales, eyes and head shape can be useful in distinguishing dangerous species from harmless ones. Some snakes found in Nepal:
Green Snakes (Orthriophis hodgsonii) have a few large scales on the top of the head and round pupils. These snakes are non-venomous and harmless. Cat-eyed Green Snakes (Boiga cyanea) have no pit organ between nostril and eye, which distinguishes them from venomous pit vipers.


Green Pit Viper (Trimeresurus septentrionalis) are the only venomous species of green snakes in Nepal. They have a pit organ between the eye and the nostril, which is an infrared detector used to find prey in the dark. Bites are painful but not fatal.
Russel Viper (Daboia russelii) is one of the most dangerous snakes in Nepal, found in the Tarai only. Its head is covered by numerous small symmetrical, oval scales, it has a long tail and long venom fangs that fold back into its mouth.


Tibet Pit Viper (Trimeresurus tibetanus) can be found in oak and rhododendron forests on Phulchoki, Helambu and in Tibet, up to 3,200m. Bites can be painful, but not dangerous.
Himalayan Pit Viper (Gloydius himalayanus) has a few large scales on the top of its head, like some non-venomous viper lookalikes. But it has a pit organ and a dark stripe from eye to mouth. Found at 1,600-3,000m in the mountains, it is active in the daytime hunting rodents. Bites can be painful but not fatal. Has been found in Mustang.


Cobra and King Cobra are common and dangerous causes of snake bite envenoming in Nepal. Most bite at dawn, injecting a large quantity of venom that leads to paralysis of the peripheral nervous system, and then death by asphyxia. Raises forebody, displays extended neck skin hood and hisses when disturbed. Found in the Tarai and up to 3,500m.
Python (Python molurus) have no venom but kill prey by constriction. They can bite if disturbed. Found mainly in the Tarai and low valleys.


Common Krait (Bungarus caeruleus), Greater Black Krait (Bungarus niger), Lesser Black Krait (Bungarus lividus) and Wall’s Krait (Bungarus walli) are the most common and dangerous causes of snake envenoming in Nepal. They differ from all other snakes in having one row of hexagonal scales along the middle of their back from neck to tail, which are much larger than other scales. Active at night, some victims do not know they have been bitten while asleep. Respiratory paralysis can kill even after 12 hours. Found up to 1,450m.
Himalayan Krait (Bungarus bungaroides) found at higher altitudes, their bites cause death due to asphyxia. Banded Krait (Bungarus fasciatus) are also highly venomous and found in the Tarai.
Cat Snake (Boiga trigonata) look like most Kraits but differ in having laterally compressed bodies, unlike Kraits, which have rounded or triangular cross-sections. Mildly venomous.


Kukri Snake (Oligodon arnensis) differs from Russell Pit Viper in having pupils that are round, large scales on top of the head and no pit organ. Unlike Kraits, it has scales on the back that are all of similar size and shape.
Common Wolf Snake (Lycodon aulicus) is a small snake that often enters homes at night to hunt geckos and mice. Unlike more dangerous Kraits, it has scales of the same size all over its body, and is harmless.


Coral Snake (Calliophis beddomei) are rare and found up to 2,200m. If cornered, it responds by flattening its body and lifting and curling its tail. Bites are rare, sometimes fatal.
Tawny Cat Snake (Boiga ochracea) are widely distributed in the Tarai and mid-hills. They are often reddish brown and active at night, but unlike Kraits are not venomous.


Water Snake are common in paddy fields and ponds, but are not venomous. The Striped Keelback (Amphiesma stolatum) is active by day and rarely bite. It has prominent and distinct spots and stripes on the body.
Adapted from:
Venomous Snakes of Nepal: A Photographic Guide
by SK Sharma, DP Pandey, KB Shah, F Tillack, F Chappius, CL Thapa, E Alirol and U Kuch
BP Koirala Institute of Health Sciences, 2013
ISBN number : 978-9937-2-6003-9
IF A SNAKE BITES
Reassure victims, lay them down sideways
Identify snake if possible
Immobilise bitten limb with splint
Do not cut, use tourniquets, ice on wound
Wash wound with soap
Transport victim quickly to a health centre with anti-venom
Symptoms
Envenoming due to cobra and krait bites lead to neuromuscular paralysis with the following effects:
Inability to open the eyes on looking up
Inability to open the mouth
Inability to protrude the tongue from the mouth
Inability to swallow
Paralysis of the muscles of the hands and feet
Difficulty breathing