
Federalism was supposed to bring the government closer to the people, decentralise medical care and improve public health at the grassroots. But the new three-tier government structure threatens to undo Nepal’s gains in improving health services.
The government’s ‘adjustment policy’ in the medical sector, which lets staff to pick their preferred tier of work, has led many to choose the federal level, leaving provinces and municipalities underserved. The biggest losers are the areas already lacking in services: Province 6 (Karnali) and the Far Western Province.
Read also:
Poor health makes Nepalis poorer, Editorial
At the Kolti Primary Health Care Centre in Bajura, there is no doctor, after the one serving here chose to be transferred to Kathmandu. Bajura District Hospital has five doctors but the contracts of three of them will soon expire.
“I have not been informed of my new hospital yet, but I am about to be transferred. In two months, there will be a shortage of doctors here,” predicts Chief Medical Officer Rup Chandra BK, adding that all technicians, including a paramedic, a radiographer and health assistants, have been transferred or will be soon.
Read also:
Is free health care possible in Nepal?, S P Kalaunee
This is how to upgrade Nepal's rural health, Sewa Bhattarai

With a population of 135,000 people, Bajura has no private hospitals and only one government hospital, a primary health care centre, and 26 health posts. WHO recommends a doctor-patient ratio of 1:1,000, but here it is 1:150,000, while Kathmandu has a ratio of 1:850.
This is nothing new: Far Western Province has long faced medical staff shortages. According to the Department of Health Services Report 2018, only 80% of positions in health facilities were filled, and only 56 of the 142 sanctioned doctor positions were staffed. That number will decrease further after adjustment.
According to a list of adjustments of 8th level general practitioners (GPs) by the ministry of health, 36 doctors were serving in Far Western Province, but only 9 of them have chosen to remain. Of the 631 doctors at this level, as many as 326 chose the federal level, which means they are concentrated in Province 3. It is the same story in all other provinces. There are only 14 doctors in Province 6.
“Far Western Province has always faced a shortage of doctors. We have a lot of nurses, assistants, and technicians, and even if they are transferred there are others to replace them. But specialist doctors earn a lot in the cities and a government hospital cannot offer them as much. No wonder they do not want to stay here if they have a choice,” says Ramesh Kunwar at the ministry of social welfare in the province.
Read also:
Poor health, Editorial
Henry Marsh returns to the institute created by his neurosurgeon colleague Upendra Devkota

The Government Doctors’ Association of Nepal (GODAN) is also unhappy. “From the beginning we have said that the medical sector is different from others and adjustment would result in neglect of underserved regions and migration of doctors to the cities, and we were right,” says Dipendra Pandey, president of GODAN. “We proposed that a federal bridge should be created, so that medical professionals working at the federal level can be sent back to their previous working area.”
Ironically, physician Govinda KC had to call off his 17th fast unto death in Dadeldhura because the district hospital did not have proper facilities in case his health deteriorated. KC has been protesting the commercialisation of medical education, which forces doctors to work in the cities to recoup their investments.
“If the government does not replace those who are leaving the province, there is going to be a great crisis in healthcare in the Far West,” says Gunaraj Awasthi, chief of the Far West Regional Health Directorate in Dipayal. “It should immediately reinstitute those medical professionals on contract service.”
Neglect kills mothers

Lalita Bohora, 27, was ten months pregnant when her husband helped her walk for three days from Kolti to Bajura District Hospital to deliver her baby earlier this year. The staff told her it was a complicated pregnancy and there were no doctors to perform a caesariean section.
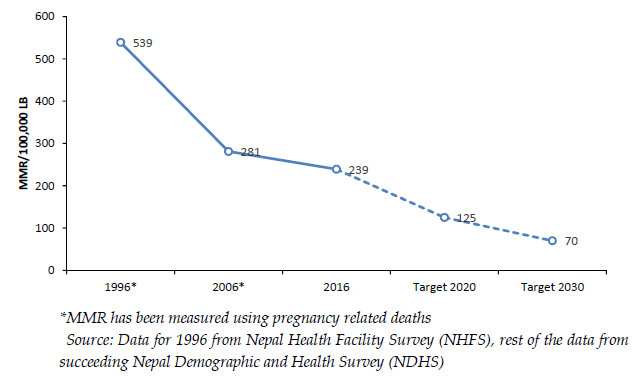
Bohora was lucky — many other mothers are in no position to walk to the district hospital. Although Nepal’s maternal mortality rate (MMR) has come down drastically from 600 per 100,000 live births two decades ago to 239 today, many mothers in remote districts like Bajura continue to lose their lives just because maternity wards are not staffed, or properly equipped.
Read also: People, Politics, and Placentas, Bikrash Gauchan
Since it started in 1997, the government’s safe motherhood program has provided cash to mothers if they do all four antenatal checkups, and mothers, and medical staff, are given cash incentives for institutional delivery. The number of birthing centres staffed by at least one skilled birth attendant has reached 1,755 nationwide.
Despite the progress, Nepal is unlikely to bring MMR down to 125 by next year as planned, or meet the Sustainable Development Goal (SDG) target of 70 by 2030. Nepal’s topography and lack of roads are not the only reasons progress in MMR has stalled. According to a recent survey, half of public health facilities in Nepal lack running water and electricity at all times.
Bajura District Hospital is constructing a new building, but it still operates out of an old, partly demolished building, where the operation theatre is a tin shed and there is irregular water supply and electricity.
“We hook up machines to the power supply during complicated operations, and the electricity suddenly goes off — we have to improvise a lot here,” says surgeon Durga Maharjan.

Ward at Bajura District Hospital
Haemorrhage during birth used to be the biggest cause of maternal mortality in the 1990s, now it is hospital-borne infections like sepsis. Many older women still think babies should be born at home, and dissuade their daughters-in-law from giving birth at a health facility.
“There is still the idea that childbirth is a normal, natural thing, and not something you need to visit a hospital for,” says Latika Maskey at the UN Population Fund (UNFPA).
Only 30% of women in Bajura go for all four of the antenatal checkups, while the average for the Far West region is 55%, and nationally it is still a high 44%. Because settlements are scattered in roadless remote Nepal, the government has focused on basic health facilities and birthing centres instead of large well-equipped hospitals, explains Punya Poudel at the safe motherhood program in the ministry of health.
“We have a roadmap to reduce MMR to 70 by 2030 by focusing on postnatal checkups, midwives will be trained for delivery and community nurses will visit women at home during ante and postnatal periods,” says Poudel.

However, many of the new birthing centres are near bigger health facilities, which makes them less useful. There is a concern among health professionals that populist agendas have fuelled construction sprees, and that the birthing centres are not always staffed and ready to provide service.
“Simply building birthing centres is not the solution. They should be properly mapped and located where they will be most effective. They should be functional so that at least one person is available 24 hours a day to provide simple delivery services,” says Pavan Agarwal at Bayalpata Hospital in nearby Achham district.
Neetu Shrestha of UNFPA says reproductive health should not be limited to treatment of birth as an event. She says: “To improve maternal health, we need to focus on sex education, invest in family planning knowledge and methods, ante and post-natal care, and address cultural barriers.”