
The Covid-19 pandemic has now killed more people than the devastating 2015 earthquake. Officially, over 9,700 Nepalis have died due to the coronavirus in the past year and a half, but the real figure is said to be at least three times more.
At a glance, it seems that densely populated urban centres with the most infections have recorded the highest fatalities. But analysing the available government data shows that the fatality rate among infected patients is higher in remote areas of the country.
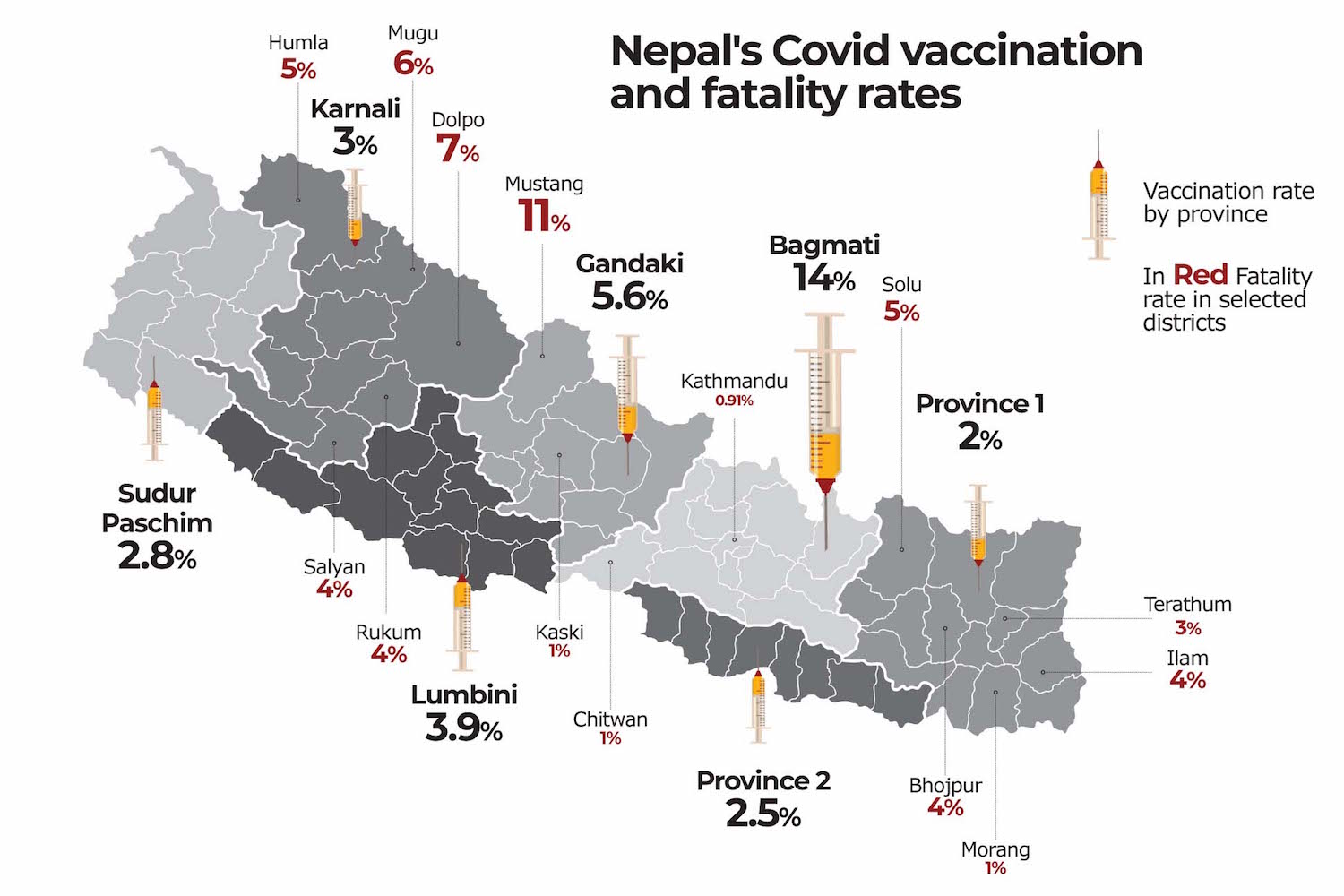
In Bagmati province, of every 1,000 Covid patients, 11.9 individuals have lost their lives, but it is 21.1 in Karnali Province. District-wise, Kathmandu saw 9.1 deaths per 1,000 cases while Mustang recorded a whopping 111.9 fatalities per 1,000.
Public health experts blame limited health care facilities in rural Nepal including ICUs, ventilators, drugs and oxygen for Covid-19 treatment for this huge discrepancy. They also have notably fewer doctors, nurses and other paramedics.
“A majority of coronavirus patients recover but most of those who died did not survive because of the lack of medical oxygen and this is also largely due to uneven distribution of health infrastructure,” says Bijay Acharya of the Massachusetts General Hospital, also associated with the US Nepal Health Foundation.
He adds: “In many places, patients have died on their way to hospitals or while being moved from one to another. Many more people in the villages have likely passed away unable to access the treatment.”
Binita Adhikari, a public health specialist affiliated with the Health Nepal Foundation and the Johns Hopkins Bloomberg School of Public Health agrees. “The fatality rate is high in remote Nepal also because many people who need treatment never reached the hospital. The Covid-19 outcome depends on how soon a person is diagnosed, hospitalised and receives treatment,” she says.
The fact that the entire Karnali Province has only two functional laboratories for Covid-19 testing (Karnali Academy of Health Sciences in Jumla and Surkhet’s Provincial Hospital) means that official figures for total cases in the region are largely under-counted. And this could also have made the fatality rate among confirmed cases higher.
Poor road infrastructure and having to travel distance, sometimes several days, for diagnosis or to access hospital care also adds to the casualties. This also means additional expenses for the poor.
The annual per capita income of people in Karnali is $606, which is nearly half of the national average, and a third of the population there is living below the poverty line. The region’s Human Development Index (HDI) at 0.538 is also much lower than the rest of the country.
Even within Karnali Province, the poorest and the most disadvantaged have been disproportionately affected. The coronavirus mortality in Karnali stands at 2.1%, but in remote Dolpo, the figure rises to 7.01%. There is just one ventilator here at the district hospital, but even that is non-functional in a lack of skilled human resources to operate it. There are only two beds with oxygen.
Similarly, the fatality rates in Mugu, Humla, Rukum East and Salyan were 6.1%, 5.15%, 4.86% and 4.07%, all much higher than the national average of 1.5%. These are also some of Nepal’s most economically and socially disadvantaged districts. Dolpo’s HDI is 0.4 and Mugu’s 0.39.
“It is very likely the total number of people infected and dying of the pandemic in the region is much higher than reported. Much of this is due to continued lack of testing and contact tracing,” says epidemiologist Lhamu Yangchen Sherpa.
Director of Teku Hospital at Kathmandu Anup Bastola agrees: “The high fatality rates in remote districts don’t necessarily mean they have more deaths, but that many of them have not had sufficient testing, which means most of the infected people barring those in critical condition didn’t reach us.”
It is however clear that regions with good health infrastructure, economically sound environment, and with higher human development index are better placed to save those infected.
While Solu, Bhojpur and Ilam saw districts 5.06%, 4.8% and 4.09% of their Covid patients succumb to the disease, Morang, Chitwan and Kaski reported only 1.02%, 1.25% and 1.52% fatality rates respectively. The figure is even lower for Kathmandu at 0.91%.
Province-wise, after Karnali, Lumbini has the highest Covid death rate at 1.77%. This is followed by Gandaki at 1.73%, with the lowest being Bagmati (1.19%).
There is also a huge disparity in Nepal’s Covid vaccination drive. Of the 1.42 million Nepalis (4.9% of the total population) who have been fully vaccinated, 55.45% of them are from Bagmati Province alone. Karnali accounts for a mere 3.5% of people who have received either both doses of AstraZeneca Covishield or VeroCell or a single shot J&J vaccine.
In other words, 14% of Bagmati residents have been fully inoculated versus 3% of Karnali people. The figure is even lower for Province 1, 2 and Far West where 2.4%, 1.71% and 2.78% of their population have been fully vaccinated.
However, some public health experts have argued that the vaccination drive when doses are scarce should not necessarily aim right now for equity, but focus on high-risk, crowded cities with mobile populations, and regions along the Indian border.
Says Bijay Acharya: “Age alone shouldn’t factor into who gets the vaccine first, economic status and social background should also be taken into account to ensure those other than the affluent also benefit. Areas with a high risk of infection and marginalised communities with poor health infrastructure should be equally prioritised.”
Nepal government is in a process procure six million dose of Pfizer vaccines for teenages from 12-18 years of age in the next six to nine months' time. Health Ministry is in the final stages of preparing -80 degree Celsius storage facilities in all seven provinces.
Translated by Sonia Awale from the original in Himal Khabar.